
{kind=link}
Dhealthwellness.com – A Glenohumeral Ligament Tear can result from a variety of causes. Although there is no one particular cause for the tear, patients often have a range of symptoms, including pain, tenderness, and instability. The most common type of dislocation occurs anteriorly, with 96% of cases caused by a force directed toward the shoulder joint while in external rotation or abduction. The second type of dislocation occurs posteriorly, and is usually caused by indirect mechanisms such as electric shock or convulsions that cause the muscles around the shoulder to contract.
Excellent Tool for Assessing Labroligamentous Pathology
MR arthrography is an excellent tool for assessing labroligamentous pathology, and has been shown to be superior to CT in the assessment of labroligamentous pathology. This technique can also provide information on labral separation and distension, and is recommended by the ACR Appropriateness Criteria. MRI images in the ABER position, when properly interpreted, can provide important clinical information about the glenohumeral ligament.
MRI scan of a 57-year-old man with superior labral tear. Note the sublabral foramen. The labrum is a structure that sits on the glenoid, and the labrum is a part of the humerus. MR images show that the labrum slips backward. This is an indication of an upper-limb fracture. This MRI scan can also detect a slipped labrum.
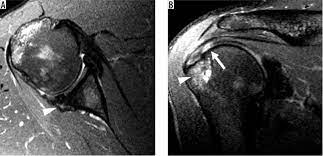
MRI is the most common diagnostic method for a Glenohumeral Ligament Tear. It uses three-dimensional imaging and fat-saturated T1 sequences to examine the shoulder. The signal intensity of a glenohumeral ligament is low, making it easier to identify. MR imaging can also reveal abnormalities in other structures of the shoulder, including the glenohumeral joint.
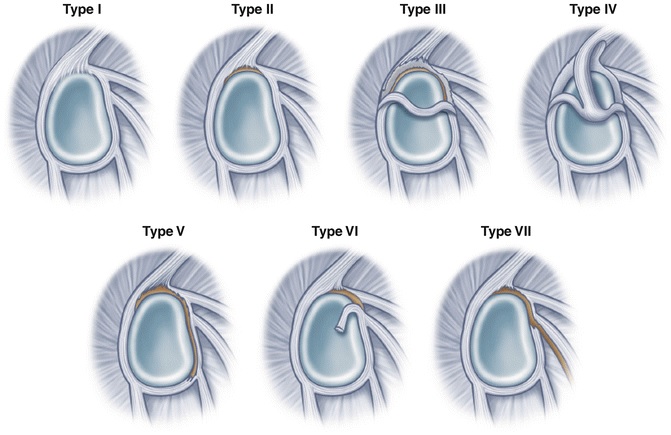
SLAP Lesions Classified Into Different Types
SLAP lesions are classified into different types based on the length of the tear. In type I, conservative treatment is necessary. While type II lesions are usually treated with conservative methods, those of type IV may require labral repair. If the tear extends to the labrum, it may be indicative of instability and may affect treatment decision-making. A labral tear may be indicative of a more serious problem, which would warrant surgery.
An MRI may show a partial volume averaging in glenohumeral ligament tears. MRI can distinguish a tear from a normal structure by careful evaluation of the entire extension of the structures. On a contrast-enhanced CT scan, a tear may show up as a single Oreo cookie in the middle of the superior labrum. A sublabral recess may also be present.
The coracohumeral Ligament is a dense fibrous structure located between the greater and lesser tuberosities of the shoulder. They provide stability to the joint capsule by preventing dislocation. These ligaments are the primary stabilizing structures of the joint. Coracoclavicular ligament, on the other hand, is composed of trapezoid and conoid ligaments and spans the clavicle. It serves to hold the clavicle in position. The acromioclavicular ligament can rupture under strong forces.
Superior Labral Anteroposterior Lesion Type IX
A type IX superior labral anteroposterior lesion occurs in a 34-year-old man with a history of trauma to the shoulder. An axial gradient-echo image of the tear shows a small fragment of the labrum partially attached to its anchor. Although the pattern of superior labral tear is complex, it most likely represents a small flap tear. This lesion often requires surgical repair and is accompanied by symptoms of pain.
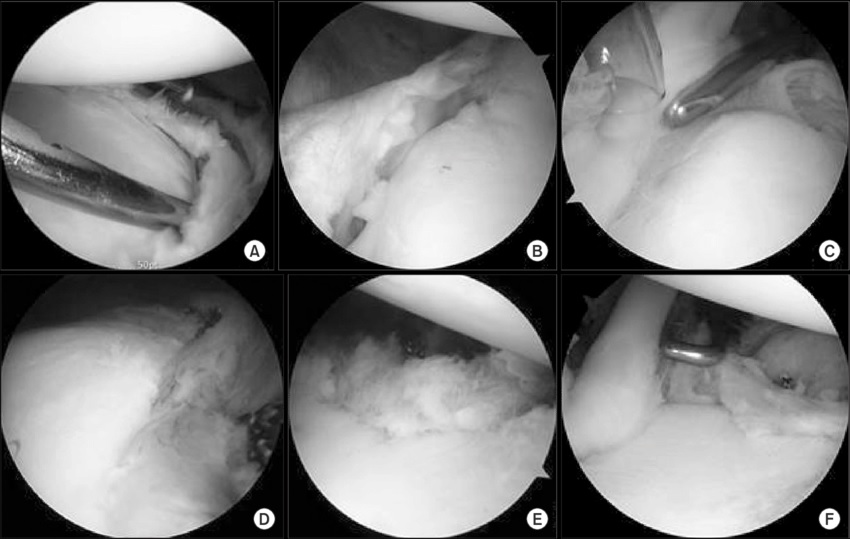
A complete Glenohumeral Ligament Tear requires an arthroscopic diagnosis. Early repair is crucial because the injury may occur more frequently than you think. If it doesn’t heal properly, it could recur. Therefore, it’s important to consult with a physician right away. While a debridement-only treatment approach may make you feel worse, it’s not always necessary. Your physician will perform an arthroscopic procedure to locate the problem and repair it.
Type I is the most common type of Glenohumeral Ligament Tear. Type II involves the labrum and the long head of the biceps tendon detaching from the glenoid cavity. A SLAP-II lesion involves both the labrum and the biceps tendon, and results in a highly mobile, inflammatory area that lacks cartilage.
Reference: